ID
105
Cancer Name
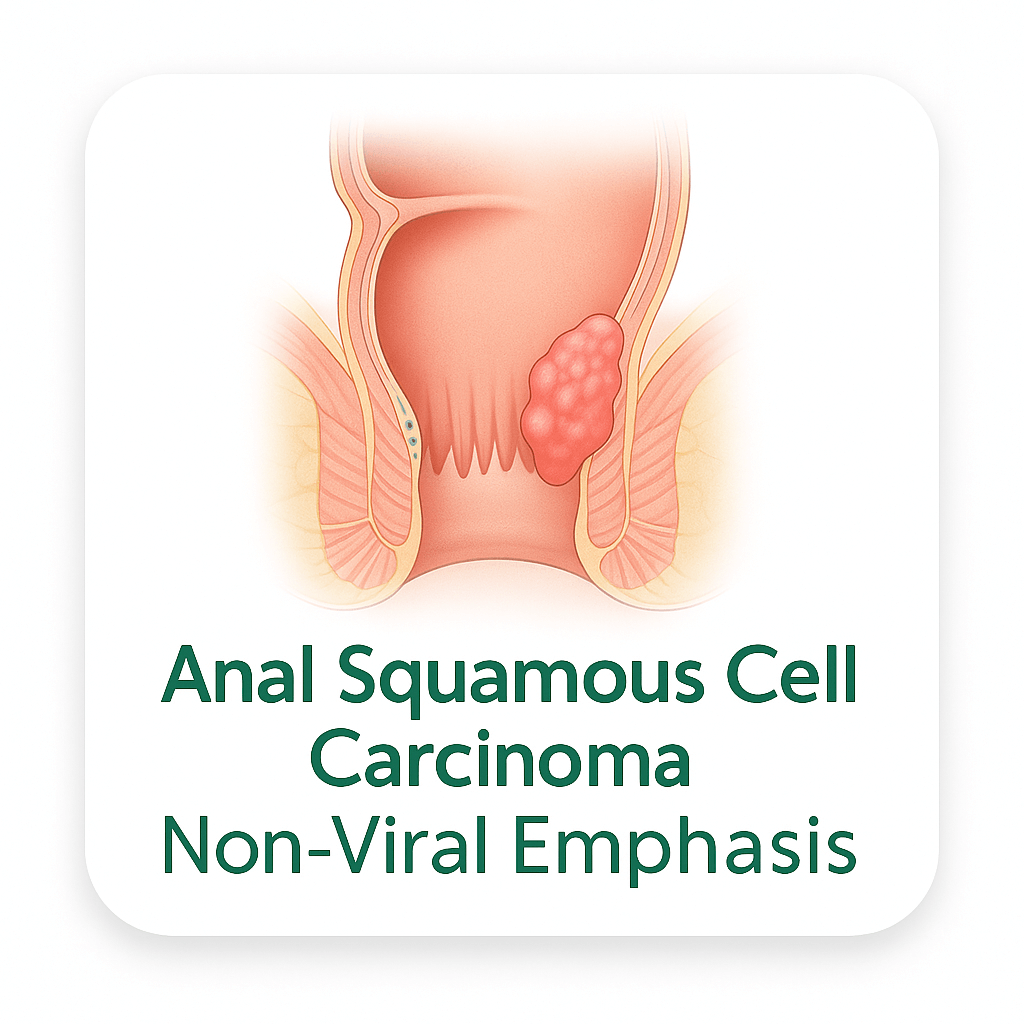
Anal Squamous Cell Carcinoma – Non-Viral Emphasis
Main Grouping
Digestive
Organ System
Anal canal
Cell Origin
Squamous epithelium
Pathways Affected
Anal squamous cell carcinoma involves a pathway landscape dominated by the PI3K/AKT/mTOR axis (PIK3CA mutations ~21-40%, PTEN loss ~10-14%), FBXW7/mTOR/c-MYC destabilization pathway (~10-13%), EGFR/MAPK/ERK overexpression (~97% EGFR), the TP53/p53 tumor suppressor pathway (somatic TP53 mutations in ~53% of HPV-negative ASCC defining the non-viral pathway), CDKN2A/cell cycle disruption, and the chronic inflammatory NF-kB signaling from the perianal microenvironment.
The PIK3CA/PI3K/AKT/mTOR pathway is the single most frequently mutated oncogenic pathway in ASCC: PIK3CA activating mutations (~21-40% — the most common somatic mutation across all ASCC regardless of HPV status, confirmed in multiple large comprehensive genomic profiling studies including the 1,844-patient FoundationOne CDx analysis) predominantly affect the helical domain at E545K (18.6% of PIK3CA-mutant cases) and E542K codons — constitutively activating the p110alpha catalytic subunit of PI3K independent of upstream RTK signaling; activated PI3K generates PIP3 at the plasma membrane recruiting AKT; AKT activates mTORC1 (through TSC1/TSC2 inhibition) driving cap-dependent translation of cyclin D1, c-MYC, HIF-1alpha, and VEGF; FBXW7 inactivating mutations (~10-13% of ASCC) compound the mTOR dysregulation — FBXW7 (F-box and WD repeat domain-containing 7) is the substrate recognition subunit of the SCF-FBXW7 E3 ubiquitin ligase complex that targets c-MYC, cyclin E, NOTCH1, mTOR, and JUN for proteasomal degradation; FBXW7 inactivation creates constitutive stabilization of mTOR, c-MYC, cyclin E, and NOTCH1 in HPV-positive TP53-wild-type ASCC; PTEN inactivating mutations (~10-14%) provide additional PI3K/AKT pathway amplification; quercetin was confirmed to inhibit PI3K/AKT/mTOR in squamous cell carcinoma cell models targeting the dominant PIK3CA-activated PI3K/AKT/mTOR pathway in ASCC; EGCG inhibits PI3K/AKT and mTOR in squamous carcinoma cell models; curcumin inhibits PI3K/AKT and mTOR in squamous carcinoma models.
The EGFR/MAPK/ERK pathway is the most consistent proliferative survival pathway across all ASCC: EGFR protein overexpression in approximately 97% of all ASCC (confirmed by IHC in large series) — a remarkably consistent finding regardless of HPV status, TP53 mutation, or grade; EGFR overexpression drives constitutive RAS/RAF/MEK/ERK and PI3K/AKT/STAT3 signaling through autocrine EGF/TGF-alpha ligand loops; EGFR also transactivates STAT3 creating anti-apoptotic (BCL-xL, MCL-1) and proliferative (cyclin D1, c-MYC) gene expression; quercetin was confirmed to suppress EGFR-mediated signaling and inhibit EMT (Slug reduction) in squamous cell carcinoma cell models (PMC7037689) targeting the EGFR overexpression dominant across ASCC; curcumin was confirmed to inhibit EGFR/Akt/ERK1/2/STAT3 in SCC-25 oral squamous cell carcinoma cells by Western blot confirmed (PMC4230161) — directly applicable to ASCC given EGFR overexpression (~97%) and squamous histology.
The TP53 pathway is the defining tumor suppressor disruption in HPV-negative ASCC: TP53 mutations present in approximately 53% of HPV-negative ASCC vs. ~4-12% of HPV-positive ASCC — this dramatic difference confirms that HPV-negative ASCC achieves p53 pathway disruption through direct somatic TP53 mutation rather than through HPV E6 oncoprotein-mediated p53 ubiquitination and degradation; TP53 mutations in HPV-negative ASCC cluster at common hotspots (R248W, R273C, R248Q, R175H) creating gain-of-function oncogenic p53 proteins; TP53-mutant ASCC also shows higher rates of CDKN2A, JAK1, FGFR1, and BRAF co-mutations confirming a distinct molecular subtype; quercetin activates p53 in squamous cancer cell models and induces apoptosis through p53-independent mechanisms in TP53-mutant cells; curcumin inhibits MDM2 restoring p53 activity.
Description
Anal squamous cell carcinoma (ASCC) is a rare gastrointestinal malignancy arising from the squamous and transitional epithelium of the anal canal, representing approximately 2 to 3 percent of all colorectal malignancies and approximately 90 percent of all anal canal carcinomas. In the United States, approximately 9,500 to 11,000 new cases of anal cancer are diagnosed annually, with ASCC comprising the dominant histological type. The incidence of ASCC has been rising at approximately 2 to 3 percent per year in the United States and United Kingdom over the past two decades. Globally, the annual incidence is estimated at approximately 50,000 new cases.
ASCC shows a clear female predominance overall (female-to-male ratio approximately 2:1 in the general population), though the male-to-female ratio is reversed in high-risk male populations. The median age at diagnosis is approximately 60 to 65 years. The incidence of ASCC rises with increasing age in the general population.
The non-viral emphasis of this template focuses on the molecularly distinct HPV-negative subset (~13-15% of all ASCC) and the non-viral carcinogenic mechanisms relevant to all ASCC beyond viral integration: HPV-negative ASCC is characterized by somatic TP53 mutations in approximately 53% of cases (vs. ~4-12% in HPV-positive ASCC), CDKN2A homozygous deletion, and HRAS mutations — features shared with cutaneous squamous cell carcinoma rather than HPV-positive anogenital squamous carcinoma; other non-viral risk factors contributing to ASCC include: immunosuppression (transplant, HIV-negative); chronic anal inflammation and fistula disease; Crohn's disease with perianal involvement; and carcinogen exposure; the non-HPV carcinogenic pathway relies on direct somatic mutation accumulation in TP53, CDKN2A, and RAS rather than viral oncoproteins E6/E7.
Across all ASCC regardless of HPV status, the dominant oncogenic pathway is PI3K/AKT/mTOR: PIK3CA mutations are the single most frequently mutated gene in ASCC at approximately 21-40% in various large cohorts, with E545K and E542K activating mutations in the helical domain predominating; FBXW7 inactivating mutations (~10-13%) stabilize c-MYC, cyclin E, and mTOR creating additional PI3K/AKT/mTOR and cell cycle amplification; EGFR is overexpressed in approximately 97% of all ASCC providing a dominant proliferative survival axis; PTEN inactivating mutations (~10-14%) further amplify PI3K/AKT signaling; PD-L1 is expressed in approximately 40-50% of ASCC reflecting immune checkpoint activation.
Overall 5-year OS by stage: stage I ~75%; stage II ~65%; stage III ~50%; stage IV ~25-30%; HPV-negative ASCC has a worse prognosis than HPV-positive reflecting more aggressive biology and resistance to standard chemoradiotherapy.
Published laboratory research confirms quercetin from onions suppressed viability of oral squamous cell carcinoma (OSCC) cells confirmed by MTT assay; induced G2/M cell cycle arrest confirmed by flow cytometry; did not affect normal keratinocytes (HaCaT and nHOK) confirmed; suppressed migration confirmed by wound-healing assay; inhibited invasion confirmed; suppressed EMT through Slug pathway confirmed by Western blot and immunofluorescence; inhibited MMP confirmed (PMC7037689) — directly applicable to anal SCC which shares the identical squamous cell carcinoma histology, EGFR overexpression (~97%), TP53 alteration, and EMT-driven invasive biology.
Plant-Based Description
Whole-food plant-based dietary patterns provide phytochemicals with confirmed activity in squamous cell carcinoma cell lines directly applicable to anal squamous cell carcinoma. Quercetin from onions and kale was confirmed to suppress viability of oral squamous cell carcinoma (OSCC) cells by MTT assay; induce G2/M cell cycle arrest confirmed by flow cytometry; not affect normal keratinocytes (HaCaT and nHOK) confirmed; suppress migration confirmed by wound-healing assay; inhibit invasion confirmed; suppress EMT through the Slug transcription factor pathway confirmed by Western blot and immunofluorescence; inhibit matrix metalloproteinases confirmed (PMC7037689) — directly applicable to anal SCC sharing identical squamous histology, EGFR overexpression (~97%), and EMT/invasion biology; curcumin from turmeric was confirmed to inhibit proliferation and invasion of SCC-25 squamous cell carcinoma cells; inhibited EGFR phosphorylation, Akt, ERK1/2, STAT3 confirmed by Western blot (PMC4230161) — targeting the ~97% EGFR overexpression in ASCC; sulforaphane activates Nrf2 targeting inflammation driving perianal carcinogenesis; EGCG inhibits EGFR and PI3K/AKT in squamous carcinoma models; apigenin induces apoptosis in squamous carcinoma cell models.
Plant Chemistry Detail
Quercetin from onions, kale, and apples has confirmed activity in squamous cell carcinoma cell lines sharing the identical histology and molecular drivers of anal squamous cell carcinoma in a published study (PMC7037689 — "Quercetin Inhibits Cell Survival and Metastatic Ability via the EMT-Mediated Pathway in Oral Squamous Cell Carcinoma") using OSCC cell lines. In this confirmed study: quercetin suppressed the viability of OSCC squamous cell carcinoma cells confirmed by MTT assay; quercetin induced cell cycle arrest at G2/M phase confirmed by flow cytometry — directly targeting the CDKN2A/p16-deficient (in HPV-negative ASCC) and cyclin E-stabilized (through FBXW7 inactivation in HPV-positive ASCC) cell cycle dysregulation; quercetin did not affect cell viability of normal human keratinocytes (HaCaT immortal keratinocytes and nHOK primary normal human oral keratinocytes) confirmed — demonstrating cancer-selective activity relevant to the anal canal squamous epithelium; quercetin suppressed OSCC cell migration confirmed by wound-healing assay — targeting the invasive phenotype of ASCC which frequently invades the sphincter complex and perirectal fat; quercetin inhibited OSCC cell invasion confirmed by invasion assay; EMT (epithelial-mesenchymal transition) suppressed through Slug pathway confirmed by Western blot and immunofluorescence — Slug (SNAI2) is a key EMT transcription factor downregulating E-cadherin and driving ASCC invasion through the sphincter; MMP activity inhibited confirmed — targeting the MMP-driven extracellular matrix degradation required for ASCC perineural invasion and lymphovascular spread; quercetin also decreased TGF-beta1-induced EMT in HaCaT keratinocyte cells confirmed — targeting the TGF-beta1 pro-invasive signaling in ASCC.
Curcumin from turmeric was confirmed to inhibit proliferation of SCC-25 oral squamous cell carcinoma cells in a dose-dependent manner confirmed; G2/M arrest confirmed; inhibited EGFR phosphorylation (Y1068 and Y1173 sites) confirmed by Western blot — directly targeting the EGFR overexpression (~97% of ASCC); Akt phosphorylation reduced confirmed; ERK1/2 phosphorylation reduced confirmed; STAT3 phosphorylation (Y705) reduced confirmed — targeting the EGFR/STAT3 axis driving BCL-xL anti-apoptotic survival in ASCC; MMP-2, MMP-9, uPA and uPAR expression downregulated confirmed (PMC4230161) — targeting EGFR/MAPK-driven invasion in ASCC. EGCG from green tea inhibits EGFR kinase by direct binding and PI3K/AKT in squamous carcinoma models targeting the EGFR overexpression and PIK3CA mutations (~21-40%) in ASCC. Sulforaphane from cruciferous vegetables activates Nrf2/ARE and inhibits NF-kB — targeting the chronic inflammatory NF-kB signaling from perianal disease (Crohn's disease, chronic fistula) contributing to ASCC carcinogenesis; sulforaphane induces p21/CDKN1A targeting CDKN2A-deleted HPV-negative ASCC cell cycle vulnerability. Resveratrol inhibits PI3K/AKT and mTOR targeting PIK3CA/FBXW7/mTOR pathway dysregulation.
Nutritional Focus
Nutritional focus in anal squamous cell carcinoma with non-viral emphasis targets the dominant PI3K/AKT/mTOR pathway (PIK3CA mutations ~21-40%, the most commonly mutated gene in ASCC), EGFR overexpression (~97%), FBXW7 inactivation (~10-13%), PTEN loss (~10-14%), and TP53 mutations in HPV-negative ASCC (~53%). Quercetin from onions confirmed to suppress squamous cell carcinoma cell viability MTT assay; G2/M arrest confirmed flow cytometry; normal keratinocyte sparing confirmed; migration suppressed confirmed; invasion inhibited confirmed; EMT via Slug suppressed confirmed; MMP inhibited confirmed (PMC7037689) — directly applicable to anal SCC squamous histology and EGFR/EMT invasion biology; curcumin from turmeric confirmed to inhibit SCC-25 squamous cell carcinoma proliferation; EGFR phosphorylation inhibited; p-Akt, p-ERK1/2, p-STAT3 reduced; MMP-2/9/uPA/uPAR downregulated confirmed (PMC4230161) — directly targeting EGFR overexpression (~97% ASCC) and PI3K/AKT; EGCG from green tea inhibiting EGFR kinase by direct binding and PI3K/AKT in squamous carcinoma models targeting EGFR overexpression and PIK3CA mutations; sulforaphane activating Nrf2/ARE and inhibiting NF-kB targeting chronic perianal inflammatory carcinogenesis (Crohn's disease, chronic fistula) and CDKN2A-loss cell cycle vulnerability; resveratrol inhibiting PI3K/AKT and mTOR targeting the PIK3CA/FBXW7/mTOR pathway dysregulation in ASCC; dietary fiber producing butyrate/SCFAs inhibiting HDAC targeting epigenetic PTEN and APC promoter hypermethylation in non-viral ASCC.
Research Notes
ASCC epidemiology: ~9,500-11,000 new US cases/year; rising ~2-3%/year; ~90% of all anal canal carcinomas; female predominance ~2:1 overall; median age ~60-65 years; stage I 5-year OS ~75%; II ~65%; III ~50%; IV ~25-30%. Non-viral subset: HPV-negative ASCC ~13-15% of all ASCC; TP53 mutations ~53% HPV-negative vs. ~4-12% HPV-positive (confirmed in multiple series); CDKN2A/p16 alterations enriched in HPV-negative (homozygous deletion); HRAS mutations only in HPV-negative in some series; HPV-negative ASCC has worse prognosis than HPV-positive; more resistant to standard chemoradiotherapy. Across all ASCC molecular: PIK3CA most frequently mutated gene 21-40% (1,844-patient FoundationOne CDx confirmed); E545K and E542K helical domain most common (37.9% and 18.6% of PIK3CA alterations); KMT2D ~16-19%; FBXW7 ~10-13%; PTEN ~10-14%; SOX2 amplification ~14%; MYC amplification ~10%; RICTOR amplification ~9%; ARID1A ~5%; APC ~4-6%; NOTCH1 ~3%; EGFR overexpressed ~97% IHC (most consistent biomarker); PD-L1 ~40-50%; PD-1 ~68.8%; TMB high (~17.1% ≥10 mut/Mb); MSI rare (~1.7%). FBXW7 inactivation stabilizes c-MYC/cyclin E/NOTCH1/mTOR — enriched in HPV-positive TP53-WT ASCC. Quercetin in OSCC squamous CC (PMC7037689): viability suppressed MTT; G2/M arrest flow cytometry; keratinocyte sparing confirmed; migration wound-healing confirmed; invasion confirmed; Slug/EMT Western blot immunofluorescence; MMP inhibited. Curcumin SCC-25 (PMC4230161): proliferation inhibited; G2/M arrest; EGFR Y1068/Y1173 phosphorylation reduced; p-Akt/p-ERK1/2/p-STAT3 reduced; MMP-2/9/uPA/uPAR downregulated confirmed.
Notes Visibility
show
Key Foods
Turmeric,Broccoli,Kale,Spinach,Brussels Sprouts,Cauliflower,Garlic,Yellow Onion,Carrot,Tomato,Beetroot,Cabbage,Blueberry,Pomegranate,Grape,Raspberry,Apple,Orange,Lemon,Soybeans,Edamame,Green Lentils,Black Beans,Chickpeas,Brown Rice,Quinoa,Oats,Wild Rice,Black Rice,Walnut,Almond,Brazil Nut,Flaxseed,Pumpkin Seeds,Chia Seeds,Sesame Seeds,Hemp Seeds,Shiitake,Maitake,Lions Mane,Cremini,Portobello,Green Tea,Ginger,Black Pepper,Garlic Powder,Parsley,Rosemary,Oregano
, Celery, Leek,Avocado,Artichoke,Radish,Tangerine, Red Onion
Linked Nutrients
vitamin-c,vitamin-e,vitamin-a,vitamin-b9,vitamin-b6,selenium,zinc,magnesium,calcium,potassium,iron,quercetin,curcumin,egcg,sulforaphane,beta-carotene,anthocyanins,dietary-fiber,l-theanine,allicin
Last Updated
2025-10-13 10:53:16