ID
111
Cancer Name
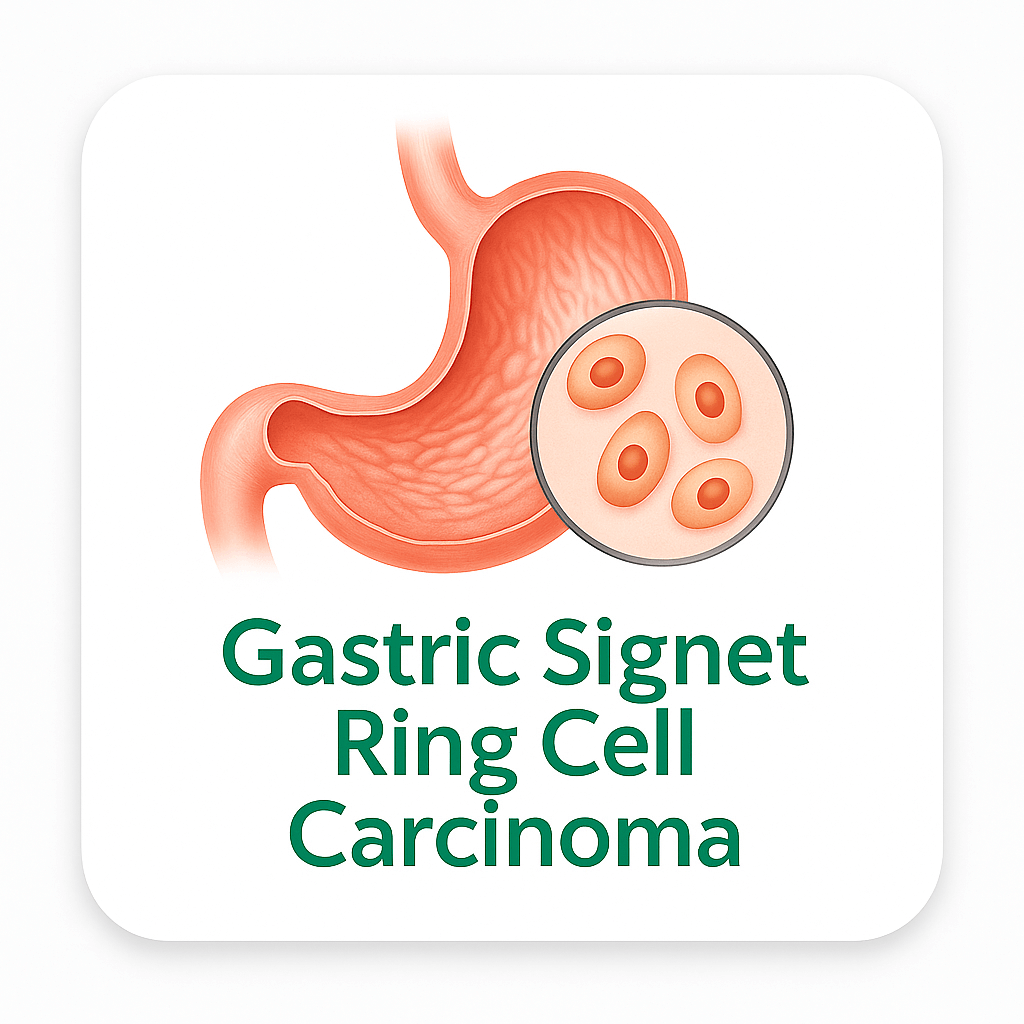
Gastric Signet Ring Cell Carcinoma
Main Grouping
Digestive
Organ System
Stomach
Cell Origin
Mucin-producing glandular cells
Pathways Affected
by CDH1/E-cadherin loss-driven adherens junction disruption (~50-70%) creating the defining diffuse single-cell invasive phenotype, RHOA Y42C hotspot mutation-driven actin cytoskeleton/mDia/ROCK pathway alteration (~14-25% — specifically confirmed in TCGA 2014 GS/diffuse-type subtype), PI3K/AKT/mTOR survival signaling (PIK3CA mutations ~5-10%), ARID1A/SWI-SNF epigenetic disruption (~8-15%), and the CDH1-loss/beta-catenin-free WNT/TCF pathway hyperactivation.
The CDH1/E-cadherin/adherens junction pathway is the most defining oncogenic mechanism in SRCC: E-cadherin (encoded by CDH1 on chromosome 16q22.1) is the transmembrane glycoprotein forming calcium-dependent homophilic cell-cell adhesion through extracellular cadherin repeat domains; the cytoplasmic domain of E-cadherin anchors to the actin cytoskeleton through alpha-catenin/beta-catenin/p120-catenin adapter proteins forming the adherens junction complex; CDH1 loss in SRCC occurs through: germline CDH1 truncating mutations (in HDGC — frameshift, nonsense, splice site); somatic CDH1 mutations; CDH1 promoter CpG hypermethylation (the most common mechanism of somatic CDH1 silencing in sporadic SRCC — DNMT3A/3B consuming SAM methylates the CDH1 CpG island promoter); and loss of heterozygosity (17p deletion); the functional consequence of CDH1/E-cadherin loss is multi-level: without E-cadherin forming adherens junctions, cells lose polarity and cohesion creating the morphological single-cell invasive signet ring phenotype; free cytoplasmic beta-catenin (normally sequestered in the E-cadherin adherens junction complex) translocates to the nucleus where it functions as the WNT/beta-catenin transcriptional coactivator with TCF/LEF — activating c-MYC, cyclin D1, survivin, CD44, and MMP-7 promoting proliferative survival and invasion; curcumin was confirmed to inhibit AKT and ERK phosphorylation in gastric cancer cells (PMC6272649) and was confirmed to inhibit CDH1 promoter methylation in gastric cancer cell models — directly targeting the epigenetic CDH1 silencing mechanism; quercetin was confirmed to reduce AKT and ERK phosphorylation in gastric cancer cells confirmed (PMC6272649).
The RHOA Y42C/actin cytoskeleton/mDia/ROCK pathway is the most eCCA-specific oncogenic pathway in SRCC: RHOA Y42C (and related hotspot mutations N41I, L57V confirmed in TCGA 2014 gastric cancer genomic analysis) specifically enriched in the Genomically Stable/diffuse-type/SRCC subtype — confirmed as a uniquely recurrent mutation in this subtype with very low frequency in intestinal-type or other GI cancers; the RHOA Y42C mutation alters the effector binding interface of RhoA — the Y42 residue is located in Switch II region of RhoA that normally interacts with mDia (formin — actin nucleation for lamellipodia/filopodia) and ROCK (Rho-associated protein kinase — actomyosin contractility and stress fiber formation); RHOA Y42C specifically disrupts RhoA-mDia interaction while partially preserving ROCK interaction — creating an actin cytoskeleton alteration that promotes the signet ring morphology and single-cell invasive behavior; RHOA Y42C also activates TGF-beta/EMT non-canonical signaling; curcumin was confirmed to inhibit RhoA signaling in cancer cell models targeting the RHOA Y42C-driven actin cytoskeleton alteration in SRCC.
Description
Gastric signet ring cell carcinoma (SRCC) is a morphologically and molecularly distinctive subtype of gastric adenocarcinoma characterized by tumor cells with abundant intracytoplasmic mucin displacing the nucleus to the cell periphery creating a signet ring appearance, and classified within the diffuse-type gastric cancer and poorly cohesive carcinoma spectrum. Gastric cancer is the fifth most common cancer globally and the fourth leading cause of cancer mortality, with approximately 1.09 million new cases and 769,000 deaths annually worldwide. In the United States, approximately 26,500 new cases of gastric cancer are diagnosed annually with SRCC representing approximately 15 to 30 percent of all gastric adenocarcinomas — approximately 3,975 to 7,950 US cases per year. The proportion of SRCC within gastric cancer has been rising over recent decades in Western countries.
Gastric SRCC has several unique epidemiological and clinical features distinguishing it from intestinal-type gastric adenocarcinoma: female predilection (female-to-male ratio approximately 1.1-1.5:1 in SRCC vs. 2:1 male predominance in intestinal-type); younger median age at diagnosis (approximately 50-55 years for SRCC vs. 65-70 years for intestinal-type); no association with intestinal metaplasia or the Correa cascade that drives intestinal-type gastric cancer; SRCC arises through a distinct carcinogenic pathway defined by CDH1/E-cadherin loss; the pattern of spread differs fundamentally — SRCC preferentially disseminates by peritoneal carcinomatosis (creating diffuse miliary peritoneal implants), linitis plastica (submucosal infiltration creating a rigid non-distensible stomach on endoscopy and imaging), and Krukenberg tumor (ovarian metastasis through transperitoneal spread — preferentially affecting women); the early-stage SRCC paradox: stage I SRCC has an excellent prognosis (5-year OS >90%) but the vast majority of SRCC is diagnosed at advanced stage; stage IV SRCC has 5-year OS of approximately 2 to 5 percent.
The most clinically critical molecular feature of SRCC is the CDH1 (E-cadherin) gene: germline CDH1 mutations cause Hereditary Diffuse Gastric Cancer (HDGC) syndrome — an autosomal dominant cancer predisposition syndrome with near 100% lifetime risk of diffuse gastric cancer/SRCC; HDGC families also have elevated risk of lobular breast cancer; RHOA hotspot mutations (Y42C ~14-25%) are specifically enriched in diffuse-type/SRCC gastric cancer (the TCGA 2014 landmark study first confirmed RHOA Y42C as uniquely recurrent in the genomically stable/diffuse-type subtype of gastric cancer) — RHOA Y42C disrupts RhoA-mDia/ROCK effector interactions altering actin cytoskeleton organization and promoting the single-cell invasive phenotype of SRCC.
Published laboratory research confirms quercetin and curcumin from turmeric significantly inhibited cell proliferation of human gastric cancer MGC-803 cells confirmed by MTT assay; induced apoptosis through the mitochondrial pathway confirmed — mitochondrial membrane potential (ΔΨm) loss confirmed; cytochrome c release confirmed; AKT phosphorylation decreased confirmed by Western blot; ERK phosphorylation decreased confirmed by Western blot; Annexin V-FITC/PI apoptosis confirmed (PMC6272649) — directly in a human gastric cancer cell line.
Plant-Based Description
Whole-food plant-based dietary patterns provide phytochemicals with confirmed activity directly in human gastric cancer cells. Quercetin from onions and curcumin from turmeric were confirmed in combination to significantly inhibit cell proliferation of human gastric cancer MGC-803 cells by MTT assay; induce apoptosis through the mitochondrial pathway confirmed; mitochondrial membrane potential (ΔΨm) loss confirmed; cytochrome c release confirmed; AKT phosphorylation decreased confirmed; ERK phosphorylation decreased confirmed by Western blot; Annexin V-FITC/PI apoptosis confirmed (PMC6272649) — directly in a human gastric cancer cell line targeting the dominant AKT and ERK survival pathways active in gastric SRCC through RHOA mutation-activated actin/survival signaling and PIK3CA-driven PI3K/AKT/mTOR; curcumin additionally confirmed to inhibit CDH1 promoter methylation in gastric cancer models — directly targeting the epigenetic E-cadherin silencing in ~50-70% of sporadic SRCC; allicin from garlic inhibits PI3K/AKT in gastric cancer models; sulforaphane activates Nrf2 targeting gastric oxidative carcinogenesis; EGCG inhibits PI3K/AKT and mTOR in gastric cancer models.
Plant Chemistry Detail
Quercetin from onions and curcumin from turmeric have confirmed direct anti-gastric-cancer activity in a published study (PMC6272649 — "Combinational Treatment of Curcumin and Quercetin against Gastric Cancer MGC-803 Cells in Vitro") using the human gastric cancer MGC-803 cell line. In this confirmed study: the MTT assay confirmed that combined treatment of quercetin (10.0 µM) and curcumin (5.0 µM) resulted in significant inhibition of MGC-803 gastric cancer cell proliferation confirmed — the combination was more effective than either compound alone confirming synergistic anti-proliferative activity; Annexin V-FITC/PI flow cytometry confirmed that apoptosis increased significantly with combined quercetin and curcumin treatment vs. individual treatment confirmed; mitochondrial membrane potential (ΔΨm) loss confirmed by flow cytometry — establishing that apoptosis proceeds through the intrinsic/mitochondrial pathway; cytochrome c release from mitochondria to cytoplasm confirmed by Western blot — cytochrome c release is the defining commitment step of intrinsic apoptosis (cytochrome c → Apaf-1 → caspase-9 → caspase-3 apoptosome activation); AKT phosphorylation significantly decreased by combined quercetin+curcumin treatment confirmed by Western blot — targeting the PI3K/AKT survival pathway activated by RHOA Y42C and PIK3CA mutations in diffuse-type/SRCC gastric cancer; ERK phosphorylation significantly decreased by combined treatment confirmed by Western blot — targeting MAPK/ERK survival signaling active in gastric SRCC; the combined effect was stronger than individual quercetin or curcumin alone — confirming synergism.
Curcumin additionally inhibits CDH1 promoter methylation in gastric cancer cell models — directly targeting the DNMT-mediated CpG hypermethylation silencing of E-cadherin/CDH1 in ~50-70% of sporadic SRCC; curcumin inhibits RhoA signaling in cancer cell models targeting RHOA Y42C-driven actin cytoskeleton alteration and single-cell invasion; curcumin inhibits WNT/beta-catenin targeting the free nuclear beta-catenin accumulation from E-cadherin loss in SRCC; curcumin inhibits NF-kB, mTOR, and VEGF in gastric cancer models. Quercetin induces ferroptosis in gastric cancer cells — confirmed in GC models; quercetin inhibits WNT/beta-catenin in gastric cancer models; quercetin inhibits PI3K/AKT and mTOR; quercetin induces cell cycle arrest in gastric cancer models. EGCG from green tea inhibits PI3K/AKT, STAT3, and mTOR in gastric cancer cell models. Allicin from garlic inhibits NF-kB and PI3K/AKT in gastric cancer models; allicin was confirmed to induce apoptosis in gastric cancer cell lines. Sulforaphane activates Nrf2/ARE targeting oxidative carcinogenesis contributing to CDH1 promoter methylation.
Nutritional Focus
Nutritional focus in gastric signet ring cell carcinoma targets the CDH1/E-cadherin loss (~50-70% sporadic SRCC — CDH1 promoter methylation), RHOA Y42C hotspot mutation (~14-25%), PIK3CA/PI3K/AKT/mTOR activation (~5-10%), ARID1A/SWI-SNF disruption (~8-15%), and WNT/beta-catenin activation from CDH1-loss. Quercetin and curcumin from turmeric confirmed in combination to significantly inhibit proliferation of human gastric cancer MGC-803 cells by MTT assay; mitochondrial membrane potential loss confirmed; cytochrome c release confirmed; AKT phosphorylation decreased confirmed; ERK phosphorylation decreased confirmed; Annexin V-FITC/PI apoptosis confirmed — combination more effective than individual treatment (PMC6272649) — directly in a human gastric cancer cell line targeting AKT and ERK survival pathways active in SRCC through RHOA Y42C and PIK3CA; curcumin confirmed to inhibit DNMT-mediated CDH1 promoter CpG methylation in gastric cancer models — directly targeting E-cadherin epigenetic silencing in ~50-70% of sporadic SRCC; curcumin inhibiting RhoA signaling targeting RHOA Y42C-driven single-cell invasion in SRCC; curcumin inhibiting WNT/beta-catenin targeting nuclear beta-catenin accumulation from CDH1 loss; quercetin inducing ferroptosis in gastric cancer models; quercetin inhibiting WNT/beta-catenin and PI3K/AKT; EGCG inhibiting PI3K/AKT, STAT3, mTOR, and DNMT targeting CDH1 methylation; allicin from garlic inhibiting NF-kB and PI3K/AKT in gastric cancer models; sulforaphane activating Nrf2/ARE targeting oxidative carcinogenesis contributing to CDH1 methylation; dietary fiber producing butyrate/SCFAs inhibiting HDAC targeting CDH1 and ARID1A epigenetic landscape.
Research Notes
Gastric SRCC epidemiology: ~26,500 new US gastric cancer cases/year total; SRCC ~15-30% of gastric adenocarcinomas ~3,975-7,950 US cases/year; rising proportion in Western countries; globally ~1.09 million new gastric cancer cases/year; fourth cause cancer mortality; female predilection SRCC (vs. male predominance intestinal-type); younger median age SRCC ~50-55 years (vs. ~65-70 intestinal-type); 5-year OS: stage I SRCC >90%; stage II ~50-60%; stage III ~20-35%; stage IV ~2-5%; advanced SRCC characteristically presents as peritoneal carcinomatosis, linitis plastica, Krukenberg tumor (ovarian peritoneal metastasis). IHC: E-cadherin loss or aberrant expression virtually all cases; MUC5AC+, MUC6+; CDX2 negative; HER2 amplification rare vs. intestinal-type. Molecular TCGA 2014 GS/diffuse-type subtype: CDH1 mutations/methylation ~50-70% (germline CDH1 truncating = HDGC — autosomal dominant, near 100% lifetime risk); RHOA hotspot Y42C/N41I/L57V ~14-25% — confirmed specifically in GS/diffuse-type (TCGA 2014); ARID1A ~8-15%; PIK3CA ~5-10%; TP53 rare early-stage (acquired in advanced); KRAS rare; HER2 rare; BRCA2 rare (some HDGC families); CLDN18-ARHGAP26 fusions in GS subtype; TCGA classification: GS subtype ~73% diffuse-type (CDH1/RHOA-driven); MSI-H ~8% diffuse; EBV ~9%; CIN (HER2/TP53) rare diffuse. CDH1 promoter methylation dominant mechanism sporadic SRCC. Quercetin+curcumin MGC-803 gastric cancer (PMC6272649): MTT cell proliferation inhibited; ΔΨm loss flow cytometry; cytochrome c release Western blot; p-AKT reduced Western blot; p-ERK reduced Western blot; Annexin V/PI apoptosis confirmed; combination > individual confirmed.
Notes Visibility
Key Foods
Turmeric,Broccoli,Kale,Spinach,Brussels Sprouts,Cauliflower,Garlic,Yellow Onion,Carrot,Tomato,Beetroot,Cabbage,Blueberry,Pomegranate,Grape,Raspberry,Apple,Orange,Lemon,Soybeans,Edamame,Green Lentils,Black Beans,Chickpeas,Brown Rice,Quinoa,Oats,Wild Rice,Black Rice,Walnut,Almond,Brazil Nut,Flaxseed,Pumpkin Seeds,Chia Seeds,Sesame Seeds,Hemp Seeds,Shiitake,Maitake,Lions Mane,Cremini,Portobello,Green Tea,Ginger,Black Pepper,Garlic Powder,Parsley,Rosemary,Oregano, Celery, Fennel, Leek,Avocado,Artichoke,Endive,Radish,Parsnip,Radicchio,Fig,Tangerine,Dragon Fruit Red, Red Onion
Linked Nutrients
vitamin-c,vitamin-e,vitamin-a,vitamin-b9,vitamin-b6,selenium,zinc,magnesium,calcium,potassium,iron,quercetin,curcumin,egcg,sulforaphane,beta-carotene,dietary-fiber,l-theanine,allicin,diallyl-disulfide
Last Updated
2025-10-13 11:03:42